Patient Safety 101
PSNet primers are regularly reviewed and updated by the UC Davis PSNet Editorial Team to ensure that they reflect current research and practice in the patient safety field. Last reviewed in 2024.
Background
The History of the Patient Safety Movement
The concept that patients could be harmed while receiving medical care has been known for thousands of years, since Hippocrates coined the phrase "first, do no harm." The term iatrogenesis—still used today to indicate harm experienced by patients at the hands of the medical system—stems from the Greek for "originating from a physician."
Although the idea of medical mistakes has been long known, the modern literature began with a famous 1956 New England Journal of Medicine paper discussing diseases of medical progress. Yet, despite research that continued to document frequent episodes of preventable harm in hospitalized patients, the safety field remained small and relatively ignored until the 1990s. The 1994 publication of the seminal commentary, "Error in Medicine," by Dr. Lucian Leape highlighted the issue and presented a framework for error analysis and prevention that is still used today. In 1999, the Institute of Medicine's To Err Is Human famously estimated that 44,000–98,000 Americans die each year due to preventable harm. Most consider its publication to represent the beginning of the modern patient safety movement. Since To Err Is Human, considerable attention has been paid to improving patient safety in hospitals, and increasingly in other settings of care as well. While much remains to be done, recent years have brought a much deeper understanding of the causes of safety issues and some progress in reducing preventable harm.
This Primer is intended to provide an overview of patient safety through defining key concepts and linking to other Primers that explore specific safety concepts in more detail.
Definitions Used in Patient Safety
The patient safety field uses the term adverse events to describe patient harm that arises as a result of medical care (rather than from the underlying disease). Important subcategories of adverse events include:
- Preventable adverse events: those due to error or failure to apply an accepted strategy for prevention;
- Ameliorable adverse events: events that, while not preventable, could have been less harmful if care had been different;
- Adverse events due to negligence: those due to care that falls below the standards expected of clinicians in the community.
Two other terms are used to describe hazards to patients that do not result in harm:
- Near miss: an unsafe situation that is indistinguishable from a preventable adverse event except for the outcome. A patient is exposed to a hazardous situation but does not experience harm (either through luck or early detection).
- Error: a broader term referring to any act of commission (doing something wrong) or omission (failing to do the right thing) that exposes patients to a potentially hazardous situation.
The Adverse Events, Near Misses, and Errors Primer discusses these terms in more detail and explores controversies regarding these definitions. The Detection of Safety Hazards Primer describes how errors and adverse events are identified and analyzed, with the goal of preventing future harm.
Epidemiology of Preventable Harm
Multiple studies have found that 10%–12% of hospitalized patients experience adverse events, with approximately half of these events considered preventable. While there is general consensus about the frequency of preventable harm in hospitals, the number of deaths that directly results from these preventable adverse events is controversial, with different studies producing widely varying estimates. This controversy arises in part because measurement of specific adverse events remains a complex and evolving area, and there is no gold standard for measuring overall safety at an institutional level. Even when an adverse event is detected, it can be difficult to determine whether the event was preventable. These concepts are discussed in more detail in the Measurement of Patient Safety Primer. Regardless, it is clear that each hospital likely has several preventable deaths per year, and a 2016 Annual Perspective explores methods by which hospitals can detect and analyze preventable deaths to try to improve overall safety.
The prevalence of preventable adverse events has not been as extensively studied in other health care settings, but a growing body of research documents that preventable harm is common in all sites of care. Most health care is delivered in the outpatient setting, and studies of outpatients have shown comparable rates of harm to those in hospitalized patients. Recent studies analyzing harm in Medicare patients in ambulatory and long-term-care hospitals have also found that more than 10% of patients in these settings experience adverse events. It has also been well documented that transitions of care are particularly risky, especially after hospital discharge. Further information on safety in these settings may be found in the Primers on Ambulatory Care Safety, Long-term Care and Patient Safety, and Transitions of Care: Challenges and Safety Practices.
The Systems Approach to Analyzing Patient Safety
Why are adverse events so common in medical care? Key insights from work in other fields have shaped medicine's response to analyzing why errors occur and informed more effective solutions to safety issues.
Traditionally, medicine treated errors as failings on the part of individual providers, reflecting inadequate knowledge or skill. However, pioneering work by British psychologist James Reason—who analyzed errors in fields as diverse as aviation and nuclear power—revealed that catastrophic safety failures are almost never caused by isolated errors committed by individuals. Instead, most accidents result from multiple, smaller errors in environments that have serious underlying system flaws. Reason's work led to the development of the systems approach, which takes the view that most errors reflect predictable human failings in the context of poorly designed systems. The systems approach seeks to identify situations or factors likely to give rise to human error and change the underlying systems of care in order to reduce the occurrence of errors or minimize their impact on patients.
Reason introduced the now-famous Swiss cheese model to describe this phenomenon. In this model, errors made by individuals result in disastrous consequences due to flawed systems—the holes in the cheese. This model is explored in more detail in the Systems Approach Primer.
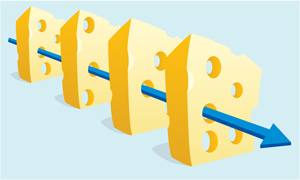
Figure. The Swiss Cheese Model of Medical Errors
It is important to note that the Swiss cheese model does not absolve individual clinicians from responsibility. Rather, it puts individual actions in the appropriate context and recognizes that the vast majority of errors are committed by well-trained, well-intentioned clinicians. As Dr. Don Berwick, the former director of the Centers for Medicare and Medicaid Services and the Institute for Healthcare Improvement, has said, "Most serious medical errors are committed by competent, caring people doing what other competent, caring people would do." Nevertheless, there is a role for individual accountability in patient safety, particularly when clinicians commit negligent acts or skirt established safety practices. The concept of just culture, now widely used in health care, emphasizes that most errors result from system flaws but also delineates where individuals should be held accountable. Further aspects of this issue are discussed in the Culture of Safety Primer and in a 2024 Perspective.
Progress and Current Challenges in Patient Safety
The seminal Agency for Healthcare Research and Quality (AHRQ) Making Health Care Safer report, issued in 2001, was the first effort to use evidence-based medicine principles in identifying practices to improve patient safety. The report galvanized patient safety efforts at hospitals nationwide and laid the foundation for further research, resulting in some of the most prominent successes in the safety field. In the past decade, thousands of lives have been saved thanks to innovative efforts to reduce health care–associated infections, prevent surgical complications, and improve teamwork among clinicians. Progress has also been made in efforts to build a climate of safety in health care, in which errors are routinely discussed and treated as learning opportunities and clinicians who are involved in errors receive support rather than blame. The AHRQ Making Health Care Safer IV report, published in 2024, added to the evidence base behind patient safety interventions, and data from AHRQ indicates that rates of preventable harm have declined significantly over the past several years.
Despite these successes, rates of preventable harm among patients remain unacceptably high, and new challenges have emerged that have hindered efforts to improve safety. One of the main new challenges to the safety field is the information technology revolution, which has transformed the day-to-day practice of medicine but has not always resulted in safer care. Some technological innovations, such as computerized provider order entry and barcode medication administration, have clearly improved safety. On the other hand, the widespread implementation of electronic medical records has often resulted in alert fatigue—and its attendant safety risks—becoming an everyday aspect of clinician workflow. Poorly designed electronic health records are frequently cited as a cause of burnout among physicians, which in itself is associated with patient safety risks.
Another challenge for the field is the need to improve safety across the continuum of care. Research in the field of patient safety began with studies of hospitalized patients. Only recently have researchers begun to analyze safety issues in ambulatory care and long-term care, and such research is starting to fill an important knowledge gap regarding effective safety interventions in these settings. More detail on safety issues in these settings may be found in the Ambulatory Care Safety and Long-term Care and Patient Safety Primers.
A final challenge relates to measurement of safety. The safety field continues to be limited by a lack of standardized measurement criteria, especially for diagnostic errors, which have not gained as much attention as other aspects of safety despite being quite common.
In response to these and other challenges, numerous organizations have developed goals and recommendations to support progress in patient safety. These organizations include the Joint Commission, the National Patient Safety Foundation, and the World Health Organization. Their efforts focus on enhancing patient and caregiver engagement, tracking and sharing safety data, promoting a culture of safety, and supporting the healthcare workforce.
Current Context
As the patient safety field has matured, investigators have gained a better understanding of the underlying causes of adverse events and methods to prevent errors. There is now a general consensus that the field should shift from focusing on single types of adverse events, and instead emphasize designing safer systems of care. This shift is based on the recognition that unsafe systems put patients at risk of multiple different types of adverse events simultaneously. For example, a patient in the intensive care unit at an academic hospital may be at risk for medication errors, several different types of health care–associated infections, and procedural complications, as well as errors related to poor communication between clinicians or inadequate supervision of trainees. The interrelatedness of these errors requires using insights from human factors engineering and other disciplines to design safer systems of care, rather than implementing targeted programs to prevent individual harms. This shift, accompanied by more rigorous measurement, will be necessary for patient safety to continue to improve.