Specimen Almost Lost
The Case
A 29-year-old woman presented to the hospital with a rash that had spread across her legs and abdomen. She was admitted to the medicine service for further evaluation and treatment of the painful, itchy rash.
To determine the etiology of the rash, she underwent a punch biopsy of her skin. The resident entered orders into the patient's electronic health record (EHR) indicating that the biopsy specimen should be sent to pathology for further evaluation. The resident also discussed the orders with the patient's nurse. The bedside nurse took the biopsy specimen to the pathology laboratory but neglected to print a copy of the resident's orders to accompany the specimen. The pathology laboratory did not have access to the same EHR as the inpatient medicine service, and the pathologist could not view the resident's orders. Without a printed copy of the orders, the biopsy specimen could not be directed to the appropriate area in the pathology laboratory for processing and analysis.
The following day, the resident attempted to look up the results of the biopsy but found none. The resident called pathology and, luckily, the laboratory had placed the specimen on hold instead of discarding it. The resident was able to print a paper order form and bring it to the laboratory so that the specimen could be processed and read by a pathologist. The patient was ultimately diagnosed with Henoch-Schönlein purpura and managed appropriately.
The Commentary
by Yael K. Heher, MD, MPH
In this case vignette, a surgical pathology specimen is nearly discarded due to inadequate communication between the treating clinical team and the pathology laboratory. This kind of error is known as a near miss, an error that has the potential to harm a patient but is caught before it reaches the patient either by diligence or by other circumstances.(1)
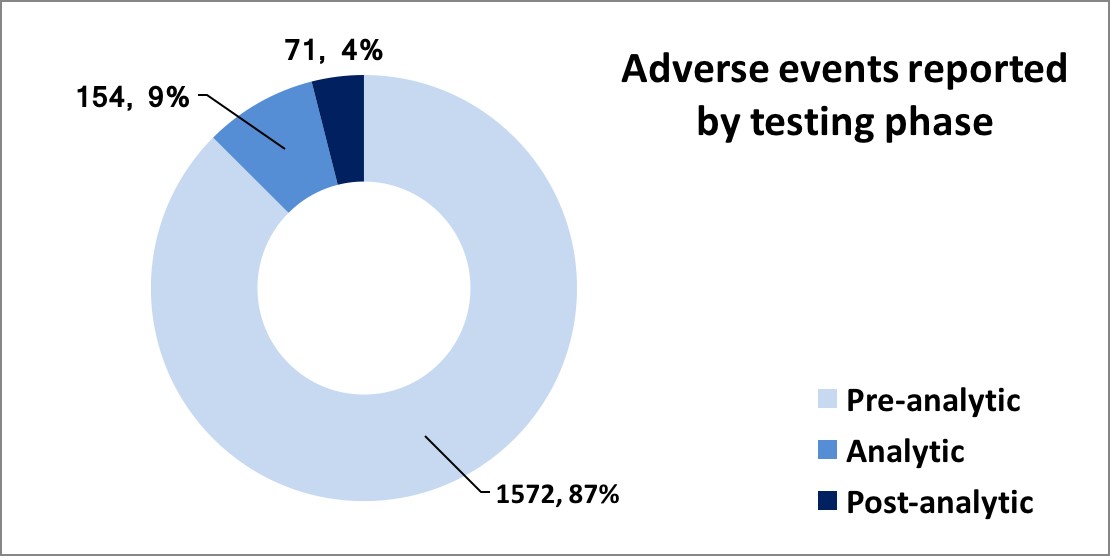
Laboratory errors are typically classified by dividing them into three phases: preanalytic, analytic, and postanalytic. Preanalytic error, as occurred in this case, typically involves the steps of laboratory testing that occur prior to the specimen actually being analyzed. This includes test ordering, transport, labeling, accessioning, triage, and access to clinical information. The rate of preanalytic error has been reported to be as high as 6% (2), making this the most common type of laboratory error.(3) In a recent unpublished review of nearly 2000 errors in our laboratory over a 2-year period, preanalytic error accounted for 87% of all errors (Figure). Despite the prevalence of preanalytic laboratory error, specimen loss is rare—the most common type of preanalytic error is specimen mislabeling. Although published rates for specimen loss do not exist in anatomic pathology, an unpublished review over a 6-year period in our center suggest a specimen loss rate of 0.002%. Discovery of preanalytic error can occur at any stage of health care delivery. Near-miss events can be caught early in the process (during specimen procurement) or late, after treatment has already been administered to the patient, and at every stage in between.
The impact of preanalytic errors on patients ranges from inconvenience to severe harm. When easily retrievable specimens such as blood or a gastrointestinal mucosal biopsy are lost, repeat testing may be unpleasant for patients but is not likely to cause long-term harm. If tests need to be redrawn or repeated, the resulting delay in diagnosis may cause a delay in treatment, minor patient harm, additional anxiety, and frustration for both patients and care providers.
In the case of an irretrievable specimen, such as a mole on the skin, a solid soft tissue nodule, or a worrisome gastrointestinal polyp, loss of the specimen results may lead to an inability to make a diagnosis and thus permanent harm. In this setting, the care team confronts a series of unanswerable questions. Did the patient have a melanoma or invasive carcinoma? What treatment would have been indicated? How confident is the treating clinician of the clinical diagnosis in the absence of a definitive pathologic diagnosis? Speculation may lead to overtreatment or undertreatment, and medicolegal liability is certainly a consideration.
To an outside observer, it may seem unfathomable that a specimen could be lost at all. However, to those familiar with the health care environment, it is well understood that laboratory operations are large, complex, and not immune to failure. Electronic health records (EHRs) and laboratory information systems (LIS) are frequently siloed, meaning that interface between these platforms make specimen tracking and reconciliation challenging. Most hospitals, regardless of their degree of digitization and automation, still retain manual processes within the laboratory that rely heavily on humans and thus fail at a predictable rate, despite competent, well-meaning personnel.(4)
Given the inherent complexity and risk associated with the laboratory ordering and testing process, it follows that clear ownership of process steps by various team members may reduce risk of error. However, handoffs and ownership of various tasks related to the processing of laboratory specimens are highly variable, both within and between institutions. Depending on the informatics infrastructure, specimens may be labeled at the point of service by the clinical team, within the pathology laboratory, or at some point in between. In addition, processes are frequently fragmented, duplicative, and manual, making them highly vulnerable to error.
Specific factors increasing the likelihood that a specimen will be lost or misprocessed are listed in the Table.(5) Laboratory errors including specimen loss occur frequently when a specimen is subject to a process outside of usual care. This may include when specimens come from unusual locations, rare tests are ordered, or special care is provided to "VIP patients." Other risk factors for specimen loss or misprocessing include reliance on individuals to do the right thing instead of robust systems, high rates of specimen handoffs, and reductions in staffing and experience.
To mitigate the risk of lost or misprocessed specimens, a range of systems solutions should be considered, including those that may be costly, such as an overhaul of the EHR and LIS to include barcoding and legal chain of custody capabilities. Ideally, an integrated EHR and LIS reduces risk by allowing pathology personnel to electronically track and reconcile specimens being processed. Treating clinicians should be able to track their patients' specimens and identify specific personnel to contact should they have questions or concerns. However, it is important to keep in mind that even robust information technology systems will not completely prevent laboratory errors. Given that specimens are still transported, barcoded, processed, and accessioned manually, risks associated with human error remain.(6)
Less costly systems solutions include the implementation of various safeguards within the laboratory. One such system is that of manual or automated specimen reconciliation between high-volume ordering providers and the laboratory. Specimen reconciliation alerts laboratory staff to pending specimens and diminishes the risk of loss by identifying missing specimens in a timely manner. Another safeguard is the implementation of specimen time outs, which can be embedded into surgical or clinical checklists.(7) The time out may include verification of labeling, review of necessary paperwork and orders, and ensuring correct provider contact information.
Within the laboratory, certain standard operating procedures can diminish the risk of specimen loss and mishandling. In our laboratory, as in the laboratory described in the vignette, specimens are held for a standard period of time if they contain inadequate information for processing. Moreover, many laboratories hold their trash for 24–72 hours in case specimens are accidentally discarded, but this is only helpful if the specimen is identified as missing prior to the trash being taken out. Additional, standard communication between the laboratory and the primary clinical team to clarify testing requests may be helpful.
In addition to systems solutions, providers and staff should receive training on appropriate specimen handling. Such training may reduce risk for a period of time, but given the complexity of test ordering, competing demands, and inherent fallibility of humans, education and training tend to be relatively weak solutions.
Review of errors associated with specimen mishandling through robust and thoughtful root cause analyses can yield important insights for health care institutions and offer targets for improvement.(8) In centers with large volumes, where losses and misprocessing events are more frequent, analyzing events to look for trends may be useful.(9) For example, are errors associated with a particular location, technical staff, or time of day? In our center, we apply the same rigorous analysis to near-miss events, with the goal of diminishing the risk of error before it causes patient harm. Auditing of processes as a part of routine quality control to seek out occult error may also be worthwhile, resources permitting.
Take-Home Points
- Preanalytic laboratory error is the most common error type and has the potential for significant patient harm.
- Specimen ordering and processing involves numerous handoffs and complex steps.
- Optimal integration of electronic health records and laboratory information systems can decrease the risk of harmful error.
- Systems solutions such as checklists, safeguards, and process standardization can improve reliability and safety.
- Thoughtful root cause analyses of near misses and errors as well as process auditing can detect and address systems vulnerabilities before they affect patient care.
Yael K. Heher, MD, MPH Director, Quality & Patient Safety Department of Pathology Beth Israel Deaconess Medical Center Harvard Medical School
References
1. McKinnon RC, eds Safety Management: Near Miss Identification, Recognition, and Investigation. New York: CRC Press; 2012. IBSN: 9781439879467.
2. Nakhleh RE. Lost, mislabeled, and unsuitable surgical pathology specimens. Am J Surg Pathol. 2003;8:98-102. [Available at]
3. Howanitz PJ. Errors in laboratory medicine: practical lessons to improve patient safety. Arch Pathol Lab Med. 2005;129:1252-1261. [go to PubMed]
4. Dekker SW, ed. The Field Guide to Understanding Human Error. 2nd ed. Hampshire: CRC Press; 2006. ISBN: 9780754648253.
5. The Truax Group. Errors in the Laboratory. Patient Safety Solutions. [Available at]
6. Becich MJ, Gilberston JR, Gupta D, Patel A, Grzybicki DM, Raab SS. Pathology and patient safety: the critical role of pathology informatics in error reduction and quality initiatives. Clin Lab Med. 2004;24:913-943. [go to PubMed]
7. WHO Surgical Safety Checklist. [Available at]
8. Slavin L, Best MA, Aron DC. Gone but not forgotten: the search for the lost surgical specimens: application of quality improvement techniques in reducing medical error. Qual Manag Health Care. 2001;10:45-53. [go to PubMed]
9. Harty-Golder B. Liability and the lab. Lost specimens. Medical Laboratory Observer. September 2007.
Table
Table. Factors Affecting the Likelihood That a Specimen May Be Lost or Misprocessed.
| Ordering and transport factors | Laboratory factors | Test and patient factors |
|---|---|---|
| Testing ordered by inexperienced provider | Times of low or inexperienced staffing (nights/weekends/holidays) | Rare test ordered |
| Off-site and non-OR specimen procurement | Lack of robust interface between LIS and EHR | Test needs to be sent out of laboratory |
| Batching during specimen transport | Lack of specimen tracking or chain of custody within laboratory | Specimen scant or minute |
| Multiple transport handoffs | Lack of specimen reconciliation | VIP patient (SOP not followed) |
OR: operating room; SOP: standard operating procedure; LIS: laboratory information systems; EHR: electronic health record.(5)
Figure
Figure. Adverse Events Reported by Testing Phase (n, %), Out of a Sample of 1797 Adverse Events.