Supervision and Entrustment in Clinical Training: Protecting Patients, Protecting Trainees
Cate O ten-. Supervision and Entrustment in Clinical Training: Protecting Patients, Protecting Trainees. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2018.
Cate O ten-. Supervision and Entrustment in Clinical Training: Protecting Patients, Protecting Trainees. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2018.
Case Objectives
- Appreciate how supervision is critical to both patient safety and trainee safety.
- Define supervision in the context of clinical training.
- Name at least four groups of factors that determine entrustment decisions for trainees.
- Explain the importance of the "zone of proximal development" for clinical training and supervision.
The Case
A 65-year-old man was admitted with head and spine trauma after falling from a tree while doing yard work. He presented with poor neurologic function requiring mechanical ventilation. A CT scan of the head and neck showed hemorrhage in his brainstem and cervical spinal cord, and he was admitted to the intensive care unit (ICU). In the ICU, his hemorrhage led to hemodynamic instability, including fluctuating blood pressures and intermittent bradycardia with heart rates as low as 20–30 beats per minute.
The decision was made to obtain a brain and spine MRI. Given the patient's critical condition, hospital policy dictated that he be accompanied by a nurse and a physician to the MRI scanner, which was 10 floors below the ICU. The ICU attending assigned the intern to transport the patient with the bedside nurse. The intern was in his second month of internship, had never done an ICU rotation before, and had never been involved in the transport of a critically ill patient.
The patient was transported to the MRI scanner. Due to some logistical challenges, he was in a holding area for more than an hour. During that time, on two occasions the patient's heart rate fell to 20 beats per minute, associated with severe hypotension. The intern, who had not been given instructions on how to manage such a scenario, did not know how to respond. Fortunately, the ICU nurse was quite experienced and appropriately administered atropine, with recovery of the heart rate and blood pressure.
The patient was finally placed into the MRI machine safely. Shortly thereafter, a chief resident came down to the MRI scanner and informed the intern that he had to leave the patient to attend a mandatory conference. The intern was hesitant given the patient's severity of illness, but the chief resident insisted that he leave. The chief resident had identified a medical student to sit in the scanner with the patient. Fortunately, there were no other clinical issues, and the patient remained stable. The medical student remained for the 2-hour scan and helped transport the patient back upstairs. Ultimately, the patient was found to have catastrophic bleeding. After discussions with his family, care was withdrawn and he died peacefully.
A week later, the intern participated in a well-being session for housestaff and discussed the events. He expressed how he was incredibly uncomfortable and felt unequipped to handle the clinical situation. He felt that he had placed the patient's life at risk because of his inexperience. He also reflected that he did not feel comfortable stating his discomfort at the time as he feared he would be labeled as weak by the attending. In addition, he shared the distress he felt when the medical student was assigned to replace him at the patient's bedside—he recognized the student likely had similar insecurities, yet neither one of them felt comfortable saying anything. He also wondered why the nurses and technicians didn't ensure that a more qualified provider was involved.
The Commentary
Commentary by Olle ten Cate, PhD
Adequate supervision is necessary in teaching hospitals to solve a constant paradox. The paradox is (i) patients deserve the best available care; (ii) the best available care is provided by experienced clinicians; (iii) but experience must emerge in trainees who start without experience; and (iv) experience requires the active care of patients.
Patients cared for in teaching hospitals should expect to receive safe and high-quality care. However, patients cannot and should not expect to always receive this care directly from the most experienced clinicians. Explaining that safe and high-quality care can be provided by a trainee requires making clear what supervision is and how the combination of an experienced supervising clinician and a trainee can and should guarantee that.
A trainee in a clinical rotation at a teaching hospital should expect to receive high-quality guidance and supervision that allows for the provision of safe, high-quality care. Trainees must be highly alert, proactive, and deliberate, especially when practicing in new environments and engaging in new clinical experiences. While they deserve adequate guidance, progression to unsupervised practice may require that they experience moments of stress, anxiety, and the need to solve problems independently.(1)
There is some confusion about the definition of supervision as applied to clinical training. Clinical supervision has been defined in the British Journal of Psychology as "The formal provision, by senior/qualified health practitioners, of an intensive relationship-based education and training that is case-focused and which supports, directs, and guides the work of colleagues (supervisees). Functions of supervision include quality control, maintaining and facilitating the supervisees' competence and capability, and helping supervisees to work effectively."(2) Kilminster and colleagues defined supervision in medical education as "The provision of guidance and feedback on matters of personal, professional and educational development in the context of a trainee's experience of providing safe and appropriate patient care."(3) Both definitions suffer from a lack of the more formal or hierarchical role description of supervision (literally to "oversee"), as reflected in common dictionaries; the latter definition omits the educational purpose of supervision in a training program. Combining these two perspectives leads me to propose a new definition for clinical supervision: The provision of guidance and support in learning and working effectively in health care by observing and directing the execution of tasks or activities and making certain that everything is done correctly and safely, from a position of being in charge.
There is an inherent tension in supervising clinical trainees, as the supervisor must be in control yet must trust learners to contribute to patient care.(4) Such entrustment decisions involve many factors, some of which the supervisor may not be actively aware of. Some factors identified by experts in the field include (i) characteristics of the learner (stage of training, specific ability, and general features, subsumed as integrity, reliability, and humility); (ii) nature of the task (difficulty, risk level); (iii) practice context (facilities, available help if needed, time of day, the need for a helping hand); and (iv) features of the supervisor him/herself (clinical experience, experience with learners, propensity to trust).(5,6) Challenging learners to engage in new clinical activities while guarding their safety and that of patients requires a delicate balance.
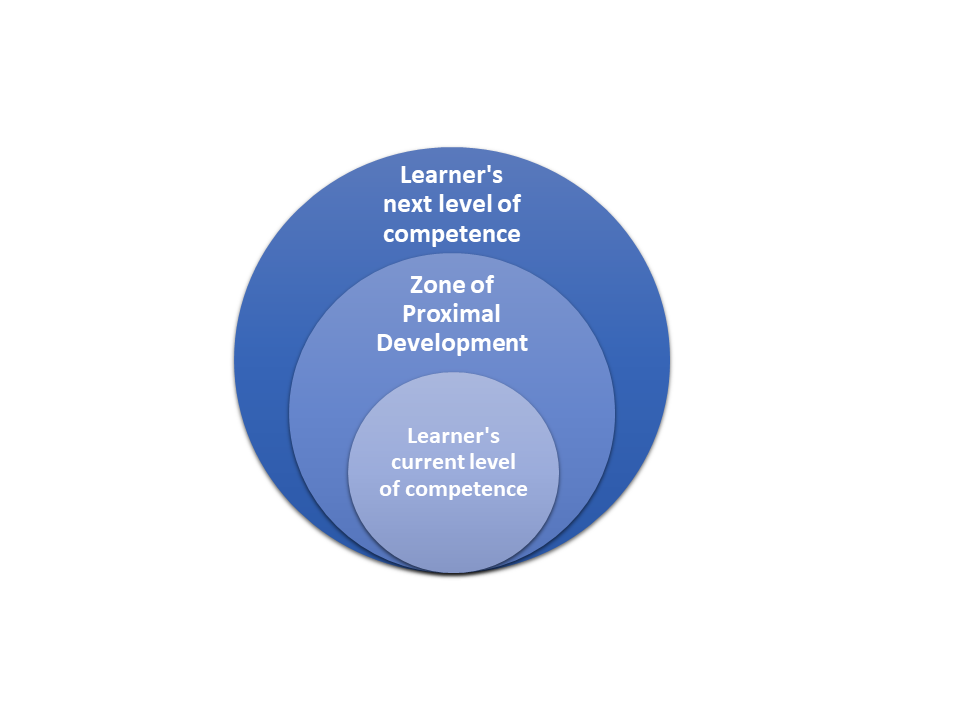
A well-known principle in educational theory, particularly relevant for supervision, is finding the right "zone of proximal development" (ZPD). In Vygotsky's words of almost a century ago, the zone of proximal development is "the distance between the actual developmental level as determined by independent problem solving and the level of potential development as determined through problem solving under adult guidance or in collaboration with more capable peers."(7) Vermunt and colleagues talk about constructive friction between teaching and learning when the zone is acceptable, and destructive friction when the zone is too big or too small. Under these latter circumstances, learning does not occur (Figure).(8,9)
Finding this balance requires agency on the part of the learner and an appropriate workplace environment.(10) The latter includes allocating sufficiently challenging tasks for the learners that will force them to exert effort but that can be mastered with some help. This may require continuous calibration, as the educational supervisor becomes more aware of the learner's capabilities.(11,12) Being in this ZPD can evoke learner anxiety but also speed up learning, as illustrated by a graduating medical student who reflected back on experiences on a nephrology rotation:
"The resident…assigned me patients right away, which was definitely disproportional, as they were very complex. It gave me more responsibility than I could bear at that moment. I discussed that, but nothing was being done. However, gradually I picked up these responsibilities, as I forced myself to call the attending specialist every time I had questions. It took another week at least to catch up with [nephrology] knowledge, but from then on my performance speeded up. My medical knowledge increased rapidly and I was surprised to see myself thrive [in role of an assistant ward attending]." (K. van Leuken, oral communication, July 2018.)
Arguably, the purpose of clinical training is the entrustment of trainees with increasing clinical responsibilities and hence a graded decrease in supervision.(13,14) Although this feels pedagogically appropriate, the efficacy of this model faces challenges. The patient safety movement has led to a variety of regulations and changes in norms that have resulted in an increase in close supervision of trainees and decrease in their autonomy.(15) While the goal of improving patient safety should not be compromised, graduates of specialty training may feel less prepared (or may actually be less prepared) to work unsupervised, leading some to take on additional training to secure continued supervision.(16-18) Patient safety may benefit in the short term, but—if graduates are unprepared for independent practice—may be harmed in the long term.
Some have argued that the only way to reconcile the need for more supervision and patient safety with the need for eventual autonomous practice is to lengthen the training period. Yet, extending training is associated with financial and logistical challenges, and prolonging programs may still not guarantee trainees will be adequately prepared. Moreover, trainees value autonomy and the absence of it may actually be a source of stress and burnout.(19,20)
There are creative approaches to balancing the tension between autonomy and supervision. For example, a model known as cognitive apprenticeship that includes supervisor roles of modeling, coaching, scaffolding, and fading (21), in which initial close supervision deliberately and gradually decreases. This cognitive apprenticeship model can offer trainees appropriate autonomy while ensuring patient safety. Using the concept of "entrustable professional activities" can provide further focus on supervision where this is most needed, and autonomy where possible.(5) Institutions and training programs should explore this and related models to ensure that they are doing all they can to get this crucial balance right—for the benefit of their trainees, as well as their current and future patients.
What Can We Say About This Case?
An intern (i) found himself very uncomfortable with an assignment; (ii) did not know what to do when unexpected events happened; (iii) felt "lucky" to have an experienced nurse at his side; (iv) felt unduly forced to leave the patient when so commanded by a chief resident; and (v) felt sorry for a medical student taking his role being even less prepared. Four others were involved: a supervisor, a nurse, a chief resident, and a medical student.
Was this a case of unsafe care from the patient's perspective? Probably not. The hospital policy to have a patient be accompanied by sufficiently experienced staff was met, as the nurse knew what to do. However, it is unclear whether an inexperienced nurse could have been assigned to the task, and clearly, two novices would have been unsafe. This should ideally have been checked among the ICU and nursing supervisors.
Was this a case of unsafe education from the intern's perspective? The intern apparently experienced destructive friction, i.e., he was asked to act beyond his ZPD. Asking trainees to act beyond their ZPD should generally be avoided; yet his perception of destructive friction can differ from one trainee to another. Given this trainee's perception of destructive friction, it is important to restore self-confidence. In this case, providing an opportunity to discuss the case in a well-being session was an excellent step.
What have could been done better? Three possible steps could have been taken: (i) The intern should have been informed about the deliberate educational purpose of choosing experiences that may be slightly beyond his comfort zone, but that patient safety is never to be compromised. (ii) The intern should have been given clear instructions on what to do in situations that feel extremely uncomfortable, if even just by providing a number to call. Briefing and debriefing is important ("What will you do when you feel uncomfortable?" and "What did you learn and what will you do in future cases?"). (iii) Wherever possible, learner autonomy should be respected. If the intern is bestowed with the responsibility to be with a patient, he should have a choice to fulfill the task satisfactorily, and not haphazardly be commanded to attend a conference. A feeling of autonomy is important to build self-confidence and intrinsic motivation.(22)
Take-Home Points
- Clinical supervision can be defined as: The provision of guidance and support in learning and working effectively in health care by observing and directing the execution of tasks or activities and making certain that everything is done correctly and safely, from a position of being in charge.
- There is a constant tension in training programs between the desire to provide the highest quality and safe patient care, while allowing for trainees to actively participate in clinical care to gain necessary skills.
- The decision to trust a trainee is driven by characteristics of the learner, risks involved in the task, practice context, the general propensity of the supervisor to trust learners, and the relationship between supervisor and learner.
- To navigate within the learner's zone of proximal development, supervisors should estimate the difficulty of tasks related to the learner's competence and preferably choose a task slightly beyond their competence to optimize the learning experience and provide the guidance needed to preserve patient safety.
- The right "dose" of supervision for critical tasks should convince patients that they receive optimal care even with less experienced learners.
Olle ten Cate, PhD Professor of Medical Education, Scientific Director of Education Senior Scientist, Center for Research and Development of Education University Medical Center Utrecht Utrecht, The Netherlands
Faculty Disclosure: Dr. ten Cate has declared that neither he, nor any immediate member of his family, has a financial arrangement or other relationship with the manufacturers of any commercial products discussed in this continuing medical education activity. In addition, the commentary does not include information regarding investigational or off-label use of pharmaceutical products or medical devices.
References
1. Dunphy BC, Cantwell R, Bourke S, et al. Cognitive elements in clinical decision-making: toward a cognitive model for medical education and understanding clinical reasoning. Adv Health Sci Educ Theory Pract. 2010;15:229-250. [go to PubMed]
2. Milne D. An empirical definition of clinical supervision. Br J Clin Psychol. 2007;46:437-447. [go to PubMed]
3. Kilminster S, Cottrell D, Grant J, Jolly B. AMEE Guide No. 27: effective educational and clinical supervision. Med Teach. 2007;29:2-19. [go to PubMed]
4. Babbott S. Commentary: watching closely at a distance: key tensions in supervising resident physicians. Acad Med. 2010;85:1399-1400. [go to PubMed]
5. ten Cate O, Hart D, Ankel F, et al; International Competency-Based Medical Education Collaborators. Entrustment decision making in clinical training. Acad Med. 2016;91:191-198. [go to PubMed]
6. ten Cate O. Entrustment as assessment: recognizing the ability, the right, and the duty to act. J Grad Med Educ. 2016;8:261-262. [go to PubMed]
7. Chaiklin S. The zone of proximal development in Vygotsky's Analysis of Learning and Instruction. In: Kozulin A, Gindis B, Ageyev VS, Miller SM, eds. Vygotsky's Educational Theory in Cultural Context. Cambridge, UK: Cambridge University Press; 2003:39-64. ISBN: 978052152883.
8. Vermunt JD, Verloop N. Congruence and friction between learning and teaching. Learn Instr. 1999;9:257-280. [Available at]
9. ten Cate O, Snell L, Mann K, Vermunt J. Orienting teaching toward the learning process. Acad Med. 2004;79:219-228. [go to PubMed]
10. Billett S. Subjectivity, self and personal agency in learning through and for work. In: Malloch M, Cairns L, Evans E, O'Connor BN, eds. The SAGE Handbook of Workplace Learning. 1st ed. London: SAGE Publications Ltd; 2013:60-72. ISBN: 9781446270523.
11. Balmer DF, Giardino AP, Richards BF. The dance between attending physicians and senior residents as teachers and supervisors. Pediatrics. 2012;129:910-915. [go to PubMed]
12. Gingerich A, Daniels V, Farrell L, Olsen S, Kennedy T, Hatala R. Beyond hands-on and hands-off: supervisory approaches and entrustment on the inpatient ward. Med Educ. 2018;52:1028-1040. [go to PubMed]
13. Dijksterhuis MGK, Voorhuis M, Teunissen PW, et al. Assessment of competence and progressive independence in postgraduate clinical training. Med Educ. 2009;43:1156-1165. [go to PubMed]
14. Kennedy TJT, Regehr G, Baker GR, Lingard LA. Progressive independence in clinical training: a tradition worth defending? Acad Med. 2005;80(suppl 10):S106-S111. [go to PubMed]
15. Halpern SD, Detsky AS. Graded autonomy in medical education—managing things that go bump in the night. N Engl J Med. 2014;370:1086-1089. [go to PubMed]
16. Napolitano LM, Savarise M, Paramo JC, et al. Are general surgery residents ready to practice? A survey of the American College of Surgeons Board of Governors and Young Fellows Association. J Am Coll Surg. 2014;218:1063-1072.e31. [go to PubMed]
17. Mattar SG, Alseidi AA, Jones DB, et al. General surgery residency inadequately prepares trainees for fellowship: results of a survey of fellowship program directors. Ann Surg. 2013;258:440-449. [go to PubMed]
18. George BC, Bohnen JD, Williams RG, et al; Procedural Learning and Safety Collaborative (PLSC). Readiness of US general surgery residents for independent practice. Ann Surg. 2017;266:582-594. [go to PubMed]
19. Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. 2016;316:2214-2236. [go to PubMed]
20. Mata DA, Ramos MA, Bansal N, et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA. 2015;314:2373-2383. [go to PubMed]
21. Collins A. Cognitive apprenticeship. In: Sawyer RK, ed. The Cambridge Handbook of the Learning Sciences. Cambridge University Press; 2005:47-60. ISBN: 9780521607773.
22. Ten Cate TJ, Kusurkar RA, Williams GC. How self-determination theory can assist our understanding of the teaching and learning processes in medical education. AMEE Guide No. 59. Med Teach. 2011;33:961-973. [go to PubMed]
Figure
Figure. Constructive Friction and the Zone of Proximal Development (ZPD).(7-9) In the ZPD, "constructive friction" is required for learning to happen. "Destructive friction" and lack of learning happens when the gap is too small or too big. Some guidance and supervision is usually needed to bridge the gap.