Near Miss with Bedside Medications
Wu AW. Near Miss with Bedside Medications. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2011.
Wu AW. Near Miss with Bedside Medications. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2011.
Case Objectives
- Understanding the definition of near miss—also known as close call.
- Appreciate the importance of close calls in reducing adverse events.
- Describe the role of incident reporting in the handling of close calls, and what should be done after discovering a close call.
The Case
A 77-year-old man on anticoagulation for a history of recent deep venous thrombosis presented to the emergency department (ED) with dizziness. In the ED, he had a heart rate of 44 beats per minute, which was felt to explain his symptoms. On further history, he revealed that he had recently increased his beta-blocker, a blood pressure medication that slows the heart.
The ED physician was concerned about the prospect of his heart rate slowing further. She ordered a syringe of atropine be placed at the bedside so it could be injected urgently if he needed it (atropine is a powerful anti-cholinergic medication that is given in emergent situations to raise the heart rate; it can cause rapid heart rate and severe confusion if used inappropriately).
Fortunately, the patient's heart rate improved while he was in the ED, and the plan was to discharge him home on a lower dose of his beta-blocker. Of note, his level of anticoagulation (i.e., his international normalized ratio [INR]) on warfarin (oral blood thinner) was found to be low. So, along with decreasing his beta-blocker dose, the plan included having him inject himself with low-molecular-weight heparin (LMWH) at home for a few days to ensure adequate anticoagulation while waiting for his INR to rise into the target range.
The pharmacist came to the ED to teach the patient how to do the subcutaneous LMWH injections, which would be required twice a day. The patient seemed to have some difficulty in understanding the medications, but the pharmacist felt comfortable with the plan to discharge him to home. She gave him 10 syringes pre-filled with the appropriate dose of LMWH to take home until he could be seen in the anticoagulation clinic.
When the patient was packing up everything from the ED, he took not only the boxes of LMWH, but also the box with the syringe of atropine that was still sitting by his bedside.
At home the next day, he tried to inject himself with the atropine but the liquid squirted all over his stomach (the atropine syringe does not have a needle as it is usually injected directly into a peripheral IV). Confused, he called the pharmacist. When the pharmacist had him spell the name on the box, she realized what had happened and had him discard the atropine. Fortunately, the patient was not harmed.
The Commentary
In this dramatic case, numerous errors occurred at multiple levels of the system. At the level of the patient, errors included the failure to recognize the difference between the atropine and LMWH, the act of scooping up the atropine with his other medications, and the fortunate failure to inject the atropine correctly. At the provider level, there was the failure to maintain the patient's INR in therapeutic range, failure by nursing staff to remove the syringe of atropine from the patient's bedside when it was no longer needed, and failure by the pharmacist to ensure patient understanding of discharge instructions. At the system level, the error involved placing drugs that might be needed by the patient's bedside with no specific orders for use. At the drug manufacturer's level, a packaging design decision led the atropine and LMWH syringes to look similar.
Fortunately, even with this confluence of errors, the patient was not harmed. This case can be defined as a near miss. Near misses are unsafe acts that have the potential to injure a patient, but do not. Different definitions are in use, which are related to two factors in describing the "near miss-ness" of an incident: whether the incident reached the patient and whether the patient was harmed. Combining these two factors yields: (i) incidents that never reached the patient, (ii) incidents that reached the patient but did not cause harm, and (iii) incidents that reached the patient and caused harm.
Near misses are perhaps more properly referred to as close calls because this allows consideration of incidents that reached the patient.(1) Category 1 and 2 cases are close calls, and Category 3 cases are "hits" (Figure 1). Thus, a common definition of a near miss is "An event or a situation that did not produce patient harm because it did not reach the patient, either due to chance or to capture before reaching the patient; or if it did reach the patient, due to robustness of the patient or to timely intervention (for example, an antidote was administered)."(2) Even more simply, some errors result in patient harm, while others do not. Close calls/near misses are errors that do not result in harm.
Frequency of near misses relative to medical errors
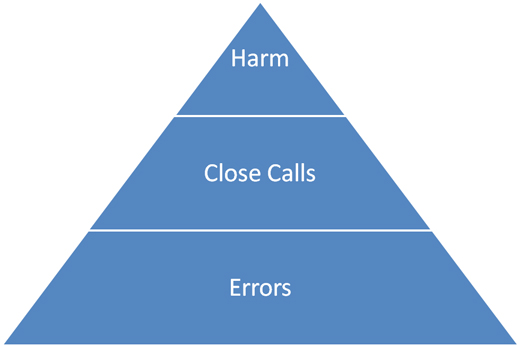
Because of the lack of systematic mechanisms to capture errors and their consequences, it is not certain how common near misses are relative to errors and to adverse events. However, it has been estimated that for each preventable death, there are between 7–100 close calls that occur before it.(3) Certainly, near misses are reported much more frequently than adverse events. For example, the Pennsylvania Patient Safety Reporting System collects more than 200,000 reports per year, 97% of which are close calls.(4) One can imagine a "safety pyramid" in which errors form the base, followed by close calls, with incidents that cause harm at the top (Figure 2).
Benefits of studying near misses
Studying close calls has several advantages over examining either medical errors or adverse events. First, they provide information on both active and latent errors in the health care system. Active errors occur where health care, usually in the form of a frontline health care worker, comes into direct contact with a patient. An example would be if a nurse were to pick up the wrong syringe and inject the patient with atropine rather than LMWH. These are generally readily apparent—unlike latent errors, which are features of an organization or design that are less apparent but that allow errors to occur. An example of this is the look-alike packaging of atropine and LMWH syringes. Importantly, the causes of close calls in health care appear to be very similar to the causes of incidents that cause harm—the same factors contribute to errors that sometimes cause harm, and sometimes do not.(5)
Second, close calls are more frequent and much more frequently reported than adverse events, providing more grist for the analytic mill. Close calls provide a more robust opportunity to examine individual practice and systems of care in error analysis. This may reveal the nature and location of what James Reason refers to as "error traps" where errors tend to recur.(2)
Third, close calls are generally less fraught with emotion and stress than adverse events. As the patient is not directly harmed, close calls are divorced from worries about liability claims. They are easier to investigate as health care staff are less paranoid about discussing errors that might have occurred. In addition, providers are less likely to be emotionally invested or involved with near misses compared to adverse events that lead to harm.
Finally, studying close calls makes it possible to identify recovery strategies in situ. Fortunately, most errors are detected before they cause harm and are corrected or mitigated. For example, the nurse discharging the patient from the ED might have asked the patient to show her/him the contents of the brown paper bag containing his medications, thereby detecting the unwanted atropine syringes. In the case of errors that go unnoticed, there is no attempt at recovery. In case of injury, there may have been no attempt at recovery, or the attempts may have been unsuccessful. Understanding recovery can lead to designing systems that are more resilient. It can also help to design systems to capture errors before they cause harm.
Identifying near misses
There are several potential ways to identify close calls. The most common methods include direct reporting by health care workers and also less obtrusive methods, such as active clinical monitoring. Patient safety reporting systems play an important role in identifying close calls. Reporting systems allow incidents to be analyzed in terms of contributing factors and to follow trends over time.
It is desirable to have multiple channels by which frontline health care workers can report incidents including close calls. These might include paper-based reporting, online reporting, email reporting, and even phone calls to a recorded hotline from clinicians who observe incidents. Online reporting to a well-publicized central system is probably most effective. Direct reporting of near misses does not have to be limited to health care workers. Patients and families can report near miss incidents.(6)
Importantly for institutions, it is not necessary to capture every incident or every near miss that occurs. Given that the true prevalence of near misses is likely quite high, capturing even a fraction of these can allow for robust analysis. In fact, capturing every adverse event or near miss can be overwhelming and may be undesirable, as in the case of repeated reporting of the same incident.(7)
Active clinical monitoring occurs when data collection about key elements of care is built into the clinical process. One example is the charting of vital signs by anesthesiologists in the operating room. Another is systematic recording by pharmacists of erroneously written prescriptions. A third is a required checklist to be completed before placement of a central venous catheter that is then added to the medical record. All of these could help to capture near misses.
The most effective methods of reporting use automated systems that continually record elements of care and can detect errors. This includes "smart pumps" (infusion pump that alerts operators when it is infusing outside of pre-configured limits), bar-code systems for medication administration and patient identification, and an increasing number of IT-based solutions. For example, a recently developed system monitors hand washing and identifies cases in which the proper hand hygiene protocol is not followed. When linked to information about the frequency of patient outcomes, these systems can identify both errors and near misses and then correlate those with patient outcomes.
How should this case be handled in an ideal world?
To derive benefit from a close call, such as the one in this case, it must be recorded or identified, analyzed, and then something must be done about it. First, the incident must be formally documented and reported, which will allow it to be examined alone and in aggregate with other incidents.(8) In this case, for example, the pharmacist involved could document the incident using the institution's patient safety reporting system.
Next, there should be a more detailed investigation of the incident. Information about the case should be collected from all of the frontline health care workers involved in the incident, including the ED physician, the ED nurse, and the pharmacist.(9,10) The investigation might even extend to questioning the patient and/or his family, as this may add a fresh perspective not readily available to clinicians.(11) The analysis should be focused on identifying common, recurring errors and systematic hazards that can be dealt with. Investigators may even want the incident to identify conditions that can be ameliorated. Interestingly, a mitigating factor identified in this case was the lack of a needle attached to the atropine syringe, which made it more difficult for the patient to self-inject.
Third, the patient safety committee or other management team should discuss the incident and analysis. It should then be assigned a priority for action, perhaps based on frequency and potential for harm. If a near miss incident occurs commonly and has a high probability to cause great harm, it may take priority over some adverse events. Solutions can then be proposed to reduce their recurrence. Specific assignment should be made for who will act to remove or mitigate risks. In this case, the patient safety committee of the hospital proposed that three actions be taken. First, the pharmacy and therapeutics committee was charged with modifying the ordering template for bedside medications to include a discontinuation time. Second, the director of ED nursing was asked to modify standard procedure so that at discharge, all medications are packed together under the supervision of a nurse. Finally, the pharmacy was tasked with adding a warning label to injectable cardioactive medications.
Finally, at a future point in time, the implementation must be evaluated. In this case, this might involve an audit to be conducted in 6 months that determines if the specified changes were made.
In conclusion, there is great power in capturing close calls as a way to improve patient safety. They represent a common, readily recorded, and relatively painless way to detect hazards. They can also identify recovery strategies that can be incorporated into designing safer care processes. In the end, close calls are not so different from adverse events. They are free lessons about how things go wrong and how they can be fixed before someone gets hurt.
Take-Home Points
- Some errors result in patient harm, while others do not. Close calls (near misses) are errors that do not result in harm.
- Close calls are much more common than adverse events, although the true incidence is not known. Because they are more frequent, they are useful to study.
- Studying close calls allows capture and analysis of recovery strategies that can help prevent harm.
- Patient safety reporting systems (incident reporting systems) are necessary to record and analyze close calls.
- To derive benefit from a close call, it must be recorded, analyzed, something must be done about it, and the intervention must be evaluated.
Albert W. Wu, MD, MPH
Director of the Johns Hopkins DEcIDE center for comparative effectiveness research
Professor of Medicine, Johns Hopkins Bloomberg School of Public Health
Faculty Disclosure: Dr. Wu is the editor of a recent book published by The Joint Commission on close calls and patient safety. Otherwise, he has declared that neither he, nor any immediate member of his family, has a financial arrangement or other relationship with the manufacturers of any commercial products discussed in this continuing medical education activity. In addition, the commentary does not include information regarding investigational or off-label use of pharmaceutical products or medical devices.
References
1. ISMP survey helps define and near miss and close call. ISMP Medication Safety Alert! Acute Care Edition. September 24, 2009;14:1-2. [Available at]
2. Wu AW, ed. The Value of Close Calls in Improving Patient Safety. Oakbrook Terrace, IL: Joint Commission Resources; 2011. ISBN: 9781599404158.
3. Institute of Medicine. Patient Safety: Achieving a New Standard for Care. Washington, DC: National Academies Press; 2004. ISBN: 9780309090773. [Available at]
4. Marella WM. Why worry about near misses? Patient Saf Qual Healthc. 2007;4:22-26. [Available at]
5. Morlock L, et al. Comparing near miss and harmful medication errors. BMJ. In press.
6. Weingart SN, Pagovich O, Sands DZ, et al. What can hospitalized patients tell us about adverse events? Learning from patient-reported incidents. J Gen Intern Med. 2005;20:830-836. [go to PubMed]
7. Wachter RM. The end of the beginning: patient safety five years after 'To Err Is Human.' Health Aff (Millwood). 2004;Suppl Web Exclusives:W4-534-545. [go to PubMed]
8. Barach P, Small SD. Reporting and preventing medical mishaps: lessons from non-medical near miss reporting systems. BMJ. 2000;320:759-763. [go to PubMed]
9. Wu AW, Lipshutz AK, Pronovost PJ. Effectiveness and efficiency of root cause analysis in medicine. JAMA. 2008;299:685-687. [go to PubMed]
10. Pham JC, Kim GR, Natterman JP, et al. ReCASTing the RCA: an improved model for performing root cause analyses. Am J Med Qual. 2010;25:186-191. [go to PubMed]
11. Millman EA, Pronovost PJ, Makary MA, Wu AW. Patient-assisted incident reporting: including the patient in patient safety. J Patient Saf. 2011;7:106-108. [go to PubMed]
Figures
Figure 1. Relationships Among Errors, Adverse Events, Close Calls, and Bad Outcomes.
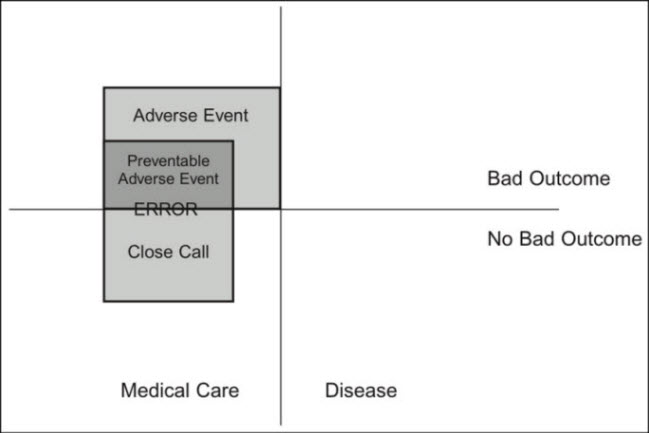
Note: The figure depicts relationships among errors, adverse events, close calls and bad outcomes. It may also be useful to examine the relationship of errors to patient outcomes. Reprinted from Wu (2), with permission of Joint Commission Resources.
Figure 2. Safety Pyramid.