Another Fall
Case Objectives
- List risk factors for falls in hospitalized patients
- Understand appropriate use of restraints
- Identify system issues contributing to falls in hospitalized patients
Case & Commentary: Part 1
A 42-year-old man with alcoholic cirrhosis, coagulopathy, thrombocytopenia, and a history of subdural hematomas (Figure 1) from falls was admitted with new bilateral subdural hematomas. The neurosurgery service drained the hematomas via burr holes. During the first week of hospitalization, the patient received a total of 45 units of fresh frozen plasma to keep his INR below 1.5 in an effort to minimize the chances of expansion of his subdural hematomas. The patient showed continued improvement and was transferred from the ICU to the step-down unit.
Falls are common in older patients, occurring each year in 35%-40% of community-dwelling persons older than 65 years. In hospitalized or institutionalized persons, falls are even more common—some studies suggest that more than 50% of nursing home residents fall annually. Injury rates are also higher in institutionalized patients, with 10%-25% of falls resulting in serious injury (fracture, laceration, or need for hospital care).(1)
Many risk factors (Table) have been described for falls,(1-4) including mobility impairment, muscle weakness, postural hypotension, visual deficits, cognitive impairment, and use of certain medications (psychotropics, class 1a antiarrhythmics, digoxin, and diuretics). Risk factors can be thought of as being intrinsic (eg, leg weakness, poor balance, cognitive impairment, visual deficit), extrinsic (eg, polypharmacy), or environmental (eg, poor lighting, loose carpets). In one study of hospitalized patients, the presence of two or more risk factors (agitation, urinary frequency, fall as presenting complaint, unstable gait, poor vision) successfully identified a group at high fall risk.(4)
The patient in this case is somewhat atypical because he is young. However, he has one of the most potent risk factors for falls: a history of more than one previous fall, with evidence of injury from the falls. There may be other contributors here as well (eg, intoxication, encephalopathy, weakness, polypharmacy), although we cannot be sure from the history.
Case & Commentary: Part 2
The patient was identified as being a fall risk. The following precautions were taken: Side rails up; Bed in lowest possible position; Call light immediately accessible; Patient told explicitly “Call nurse if you need anything”; Patient placed in area with many nurses nearby; Bed alarm activated. The patient stated he did not want to be restrained, and staff believed him to be competent. The next evening the patient attempted to climb out of bed by squeezing between the bed rails (Figure 2) and fell to the ground.
Various strategies are used for fall prevention in the hospital. Perhaps the most common strategy is the use of restraints, including physical restraints (eg, wrist restraints, vests, bed rails) and chemical restraints (ie, psychotropic medications). At the other end of the spectrum are multifactorial interventions involving comprehensive structured individual assessments, which attempt to identify and modify known risk factors for falls. These multifactorial interventions include such components as education of staff, review and modification of medications (especially psychotropic medications), institution of exercise and balance training, and modification of environmental hazards. Still other strategies, many of which were implemented in this case, rely on specific interventions to prevent falls or mitigate their damage when they occur: bed alarms to notify staff when a patient attempts to get out of bed; moving the patient to a room close to the nursing station; obtaining a sitter for agitated patients who appear to be at high fall risk; and moving the patient’s mattress to the floor. The last strategy (moving the mattress to the floor) is one of my favorites, because it is a simple and direct maneuver that eliminates the risk of serious trauma that might be sustained if an agitated, unstable patient tried to climb out of bed. It is, however, frequently challenging to implement because it is perceived as making tasks more difficult for doctors and nurses (since they have to bend to reach the patient) and as being less clean.
Unfortunately, the evidence to support any particular fall reduction strategy in the hospital is quite weak,(1,5,6) and many interventions can be promoted only on the basis of their face validity. Although multi-component/multifactorial interventions have been shown to work both in the community (7) and in nursing homes,(8) no good randomized controlled trials have yet demonstrated their efficacy in the hospital. The evidence for other more specific interventions is also lacking.
This patient specifically stated that he did not want to be placed in restraints. The use of restraints poses special concerns.(9-16) First, there is the obvious consideration relating to the unwanted, sometimes violent, infringement of individual liberty and autonomy. Developing adequate safeguards to ensure appropriate use of restraints is a major task in hospitals. Second, substantial evidence indicates that restraint use can harm, and occasionally kill, patients.(14-16) Use of physical restraints does not reduce serious injury (9); in fact, the literature suggests that just the reverse is true.(11-13)
Bed rails form an important subcategory of physical restraint. The use of bed rails is ubiquitous, and they are frequently perceived as innocuous mobility aids that do not restrain the patient. However, most experts consider bed rails a form of restraint that can restrict freedom of movement. In fact, patients may injure themselves more seriously by trying to climb over bed rails than by simply getting out of bed (as in this case), and there are case reports of fatal patient entanglements in bed rails.(15)
Coagulopathic patients may represent a patient category in whom special precautions are warranted. However, the presence of coagulopathy alone should not justify restraint use. For this particular coagulopathic patient, several commonsense steps appear to have been taken to reduce the risk of falls (for instance, placing the bed in the lowest possible position). Nonetheless, bed rails were used in spite of the patient’s wish not to be restrained. Bed rails should only be used in select instances, such as for the specific purpose of facilitating bed mobility in patients with weakness (eg, after a stroke) who are receiving rehabilitation or in sedated or somnolent patients who are on life-sustaining treatments. Given the information presented, I do not think bed rails should have been used for the patient in this case. Although some nurses or physicians may resist the idea of leaving the rails down in the confused or agitated patient, this case, in which the fall actually occurred while the patient was trying to climb out of bed by squeezing between the bed rails, demonstrates why this strategy is well worth considering. Each of the other five interventions was entirely appropriate.
Case & Commentary: Part 3
The patient was found on the floor with no sign of injury. He agreed to be placed in a Posey overnight. Two days later, he was transferred to the medical ward. The nurses identified him as being at “very high risk” for falls and thought the patient should be placed in restraints. However, he adamantly refused. The staff again believed the patient to be competent and therefore did not feel they could restrain him against his will. No psychiatric evaluation was requested.
Sidebar: Medicolegal Issues in the Use of Restraints by: Bryan Liang, MD, PhD, JD
The use of restraints in hospitals is controversial. Most accreditation and advocacy groups strongly recommend use of other means if at all possible.(1,2) Although generally used to prevent injury from falls, restraints may also cause injury. From a legal perspective, physical restraints that result in injury may lead to a lawsuit adjudicated under the standard medical malpractice negligence rule. This rule generally requires a patient-plaintiff to show a breach of the relevant standard of care. If the standard (as usually determined by expert testimony) is that the patient, when taking into account all relevant clinical and sociomedical circumstances, was a risk to himself or others in the hospital, restraints may be deemed justified.
Alternatively, the patient’s attorney may choose to have the suit heard under a general negligence rule. This latter circumstance would not require a professional standard of care to define what is acceptable. Rather it would rely on a layperson’s determination of whether use of restraints in the specific circumstance was "reasonable." Since use of restraints is a very emotional issue and would be evaluated in hindsight, providers may risk significant liability under this kind of general negligence suit.
Restraint use against a patient’s wishes is generally justified only when a professional assessment of the patient indicates that he or she is likely a risk to him or herself and/or others.(3,4) Such a determination is often linked to an assessment of mental competence, and a relevant consultation (usually by a psychiatrist) should be obtained for this evaluation. However, a patient who is a risk to him or herself or others does not need to be deemed permanently incompetent to be restrained; even temporary incompetence (for example, due to pharmacotherapy or alcohol abuse) may justify involuntary restraint. It is critical that all providers document findings regarding competency and recommendations for restraints carefully in the chart. Failure to do so may result in litigation for false imprisonment, a very serious cause of action, which could subject the provider to liability, including an award of punitive damages. Of course, providers who negligently ignore a patient’s repeat falls might also be subject to liability. Thus, careful risk assessment and competency evaluation are imperative in cases where involuntary restraints are considered.
Overall, in this case, it appears that the patient was competent, and thus providers would not likely be able to override his wishes regarding restraints. However, it would be prudent for providers to obtain a psychiatric consultation to test this conclusion, particularly because of the high risk of repeat falls that were identified by various providers during the patient’s care.
References
1. American Geriatrics Society. Position Statement: Guidelines for Restraint Use. 1991. [ go to related site ]
2. JCAHO. Long-Term Care Standards Manual (1996), Standards RI.2.6 (defining restraint), TX.8 (emphasizing a restraint-free environment), TX.8.1 (requiring restraint alternatives and safe, appropriate restraint use when alternatives prove ineffective).
3. Sarno GG. Civil liability for physical measures undertaken in connection with treatment of mentally disordered patient. In: American Law Reports. 4th ed. Rochester, NY: Lawyers Co-op Pub. Co.; 1981:464-509.
4. Sheline Y, Nelson T. Patient choice: Deciding between psychotropic medication and physical restraints in an emergency. Bull Am Acad Psychiatry Law. 1993;21:321-9.
Case & Commentary: Part 4
That evening the patient fell for a second time while trying to get out of bed. He was found on the floor, bleeding from his mouth. There were no new neurological findings. A repeat head CT showed no increase in the size of the subdural hematomas. The lip laceration was stitched and the patient was placed in restraints, over his objection.
Upon further investigation, the following factors were identified as contributing to this patient’s repeat fall: the floor nurses were not aware of the patient’s previous fall in the step-down unit; efforts to place the patient in a room closer to nurses failed due to a lack of available beds near the nursing station; no high volume bed alarms were available and those in use were not loud enough to hear outside a patient’s room; and sitters were not available due to budget restrictions.
The case presentation identifies several factors as contributors to the patient’s fall on the medical ward. All of them are amenable to improvement. The first, and in my view most important, systemic weakness in this case is the lack of communication from one team to another. In my experience, this is an extremely common problem throughout our health care system, affecting the quality and safety of care at multiple transition points. These transition points may lie between or among hospital teams or units, as in this case (including such transitions as moving from the emergency department to the floor, or from the floor to the diagnostic imaging suite), or between the nursing home and the hospital. Concerted efforts at the institutional level must be made to identify critical information elements that must be transmitted with a patient, and to define explicit and standardized mechanisms for the reliable transmission of these information elements.
One solution to enhance communication would be to use identification bracelets to notify caregivers of fall risk. This intervention is inexpensive and easy to implement, and has been studied; evidence for effectiveness is lacking, however.(17) Another solution might be to develop a checklist of safety-related information (eg, vision impairment, hearing impairment, cognitive impairment, weight-bearing limitations, allergies, and falls history, etc.) to be transmitted from unit to unit or provider to provider. In this case, automatic transmission of the history of a previous fall (one of the strongest risk factors for future falls) by some mechanism may have prevented the second fall.
Many institutions may face financial or personnel constraints that make implementation of fall prevention strategies challenging. These obstacles must be addressed one by one. Moving high-risk patients closer to the nursing station may be inconvenient for staff; the inconvenience should be recognized and mitigated. Adequate bed alarms can be purchased, but some administrators may hesitate given the lack of controlled trials supporting their use.(5) Persuasion by opinion leaders among the medical staff may be necessary. Finally, the lack of sitters could be addressed in some instances by having family members sit with a patient or by rethinking the budget allocation.
Two final thoughts occur to me as I review this case. First, although falls have been studied extensively in the community and in nursing homes, there is little high quality research on fall prevention in the hospital. The absence of compelling evidence for different strategies hinders the adoption of formal fall prevention programs. The number and variety of potential interventions should make fall prevention in the hospital a fruitful area of investigation.
Finally, falls are necessarily linked with mobility. Impairment in mobility is itself a serious problem in the hospital, putting patients at risk for many other problems, including delirium, pressure ulcers, and functional decline. The need to maintain or regain mobility is often counterbalanced by the increased risk of falls that comes with increased mobility. Every time a weak or frail patient walks, he or she may be at risk of falling. Walking, however, is critical to patients’ well-being. Thus, we must acknowledge this risk while actively trying to reduce it. One cannot eliminate all risk of falls, but one can institute measures to prevent falls or minimize their damage when they occur (for example, there is solid evidence for the efficacy of hip protectors in preventing hip fractures,(5) but this represents a change in emphasis from fall prevention to attenuation of trauma from falls). The great challenge is to design these measures so that they do not hinder the process of regaining mobility and avoid the cascade of functional decline that results from limiting mobility.
Sidney T. Bogardus, Jr., MD Yale University School of Medicine
Faculty Disclosure: Dr. Bogardus has declared that neither he, nor any immediate member of his family, has a financial arrangement or other relationship with the manufacturers of any commercial products discussed in this continuing medical education activity. In addition, his commentary does not include information regarding investigational or off-label use of pharmaceutical products or medical devices.
References
1. Anon. Guideline for the prevention of falls in older persons. J Am Geriatr Soc. 2001; 49:664-672.[ go to PubMed ]
2. Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med. 1988; 319:1701-1707.[ go to PubMed ]
3. Nevitt MC, Cummings SR, Kidd S, et al. Risk factors for recurrent nonsyncopal falls. A prospective study. JAMA. 1989; 261:2663-2668.[ go to PubMed ]
4. Oliver D, Britton M, Seed P, et al. Development and evaluation of an evidence-based risk assessment tool (STRATIFY) to predict which elderly inpatients will fall: case-control and cohort studies. BMJ. 1997; 315:1049-1053.[ go to PubMed ]
5. Agostini JV, Baker DI, Bogardus ST. Prevention of falls in hospitalized and institutionalized older people. In: Shojania KG, Duncan BW, McDonald KM, Wachter RM, eds. Making Health Care Safer: A Critical Analysis of Patient Safety Practices. Evidence Report/Technology Assessment No. 43, AHRQ Publication No. 01-E058; July 2001. [ full report available ]
6. Oliver D, Hopper A, Seed P. Do hospital fall prevention programs work? A systematic review. J Am Geriatr Soc. 2000; 48:1679-1689.[ go to PubMed ]
7. Tinetti ME, Baker DI, McAvay G, et al. A multifactorial intervention to reduce the risk of falling among elderly people living in the community. N Engl J Med. 1994; 331:821-827.[ go to PubMed ]
8. Ray WA, Talyor JA, Meador KG, et al. A randomized trial of a consultation service to reduce falls in nursing homes. JAMA. 1997; 278:557-562.[ go to PubMed ]
9. Tinetti ME, Liu W-L, Ginter SF. Mechanical restraint use and fall related injuries among residents of skilled nursing facilities. Ann Intern Med. 1992; 116:369-374.[ go to PubMed ]
10. Marks W. Physical restraints in the practice of medicine: current concepts. Arch Intern Med. 1992; 152:2203-2206.[ go to PubMed ]
11. Ejaz FK, Jones JA, Rose MS. Falls among nursing home residents: an examination of incident reports before and after restraint reduction programs. J Am Geriatr Soc. 1994; 42:960-964.[ go to PubMed ]
12. Evans LK, Strumpf NE, Allen-Taylor LS, Capezuti E, Maislin G, Jacobsen B. A clinical trial to reduce restraints in nursing homes. J Am Geriatr Soc. 1997; 45:675-681.[ go to PubMed ]
13. Hanger HC, Ball MC, Wood LA. An analysis of falls in the hospital: can we do without bedrails? J Am Geriatr Soc. 1999; 47:529-531.[ go to PubMed ]
14. Miles S. A case of death by physical restraint. New lessons from a photograph. J Am Geriatr Soc. 1996; 44:291-292.[ go to PubMed ]
15. Parker K, Miles SH. Deaths caused by bedrails. J Am Geriatr Soc. 1997; 45:797-802.[ go to PubMed ]
16. Rubin BS, Dube AH, Mitchell EK. Asphyxia deaths due to physical restraint. A case series. Arch Fam Med. 1993;2:405-408.[ go to PubMed ]
17. Mayo NE, Gloutney L, Levy AR. A randomized trial of identification bracelets to prevent falls among patients in a rehabilitation hospital. Arch Phys Med Rehabil. 1994; 75:1302-1308.[ go to PubMed ]
Table
Table. Risk Factors for Falls in the Hospital
| Fall as presenting complaint or history of falls |
| Mobility impairment or unstable gait |
| Muscle weakness |
| Use of assistive devices |
| Postural hypotension |
| Visual deficits |
| Cognitive impairment |
| Agitation |
| Urinary frequency |
| Medications (eg, psychotropics, class 1a antiarrhythmics, digoxin, and diuretics) |
| Environmental factors (eg, poor lighting, loose carpets) |
| Arthritis |
| Depression |
| Age > 80 years |
Figures
Figure 1. Subdural Hematoma
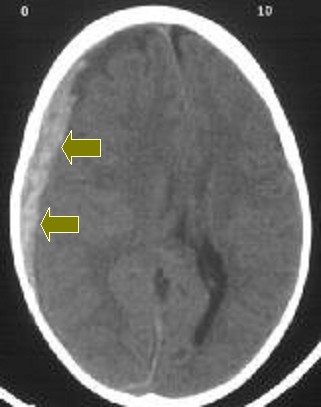
Figure 2. Patient Caught in Bedrails
