In Conversation with… Edward Tenner, PhD
Editor's note: Edward Tenner is an independent writer, speaker, and consultant on technology and culture. He received his PhD from the University of Chicago and has held visiting positions at Chicago, Princeton, Rutgers, the Smithsonian, and the Institute for Advanced Study, as well as a Guggenheim Fellowship. His book Why Things Bite Back: Technology and the Revenge of Unintended Consequences is a seminal work in patient safety and is generally credited with introducing the concept of unintended consequences, including those surrounding "safety fixes," to a general audience. His most recent book is Our Own Devices: The Past and Future of Body Technology. He is completing a new book on positive unintended consequences.
Dr. Robert Wachter, Editor, AHRQ WebM&M: What do you mean by the term unintended consequences?
Dr. Edward Tenner: I mean consequences that are not just disadvantageous but are actually inimical to the purpose that one originally had. A revenge effect goes beyond a side effect. It isn't only an unfortunate result of a therapy with benefits that outweigh it. It's a result that cancels out the reason for doing something.
RW: Can you give us your favorite example or two from outside of health care?
ET: One typical one that bridges health care and consumer behavior is the filter cigarette. Smoking one is really just as unhealthy as smoking an unfiltered cigarette because of the way the smoker compensates for lower nicotine by inhaling more deeply. That is a frequent theme: people tend to offset the benefits of some safety measures by behaving more dangerously. I don't agree with a few risk analysts who see this behavior as a universal law: automobile seat belts actually do reduce deaths and injuries, although the record of, for example, antilock brakes is less clear. But it's common for safety technology to backfire.
RW: So when you've written about "revenge effects"—that seatbelts or airbags cause people to go faster. First of all, are they so anticipatable that we should just now expect them? Second, how do you decide then whether the intervention is going to have a net positive effect?
ET: Trying to prevent all revenge effects has revenge effects of its own, so I don't subscribe to the strong form of the precautionary principle, that you shouldn't try anything new unless you're sure it's harmless. This can mean locking in existing revenge effects. In the case of seatbelts and other road technology, I just read in The New York Times about how the latest airbags may be more dangerous for drivers who are using their seatbelts. Airbag inflation sufficient for an unbelted person or a large person may seriously injure a person wearing a seatbelt, a child, or a smaller person.
RW: We're going to segue into health care; let me do it via aviation, which is a common theme in patient safety. You have undoubtedly seen discussions that say that the modern cockpit has become so automated that pilots are lulled into a sense of security and no one's on the till anymore. What do you think about that general philosophy—that although automation may be good, one of the unintended consequences will be that people stop paying attention?
ET: I think that risk has always been there. In fact that risk was used in the 19th century to oppose safety signals on railroads. People said that if you had these red and green lights, the engine drivers would just pay attention to the lights and they would neglect their senses. There is a problem that arguments like that have been used against all kinds of really beneficial systems that we take for granted today. I think that it's really a matter of constant training and practice to be able to work in an unsupported or semi-supported mode. It's an organizational problem more than a technological one. I don't think the existence of something that's automated necessarily leads to the abandonment of skills, although the tendency is clearly there.
RW: I'm told that TSA airport screeners are periodically shown an image of a weapon in a suitcase just to be sure that they're awake. Can you envision technological fixes built in to health care to create some almost artificial vigilance?
ET: I don't think it's necessarily a bad idea. The big problem is how far you are willing to go financially in continuing to train people and have people practice to be able to work if the system fails. We saw that in the landing in the Hudson, here was a pilot who was widely considered to be "old school," so the question was raised whether younger pilots who are coming on now would have the same ability to work with the system. Of course some people have also disputed how skilled Captain Sullenberger really was; some people are second-guessing him, saying it might have been safe to go back and land, etc. But it's clear that the public wants heroes, people who can improvise when the automated systems fail, who can somehow pull off a miracle and get the job done.
RW: Checklists are a very hot issue in health care, the idea that things that we've relied on human memory for, we're now trying to encode in a series of manageable steps. What unintended consequences should we be on the lookout for as we think about that as a new strategy?
ET: I like the idea of checklists up to a point. But I'm worried about checklists because they make the assumption that all cases are basically very similar, and that's a normal assumption for professionals. A professional really needs to work to some kind of list of best practices, but on the other hand, when people look at the very best professionals, they're the people who very often have the ability to see something that's different in this case and to investigate it further. I know that in the current medical system that is very hard to do given the workloads and systems of reimbursement, so I'm not blaming people for not being full-time problem solvers. What makes me uneasy about the checklists is the assumption that there is a body of best practices and you just follow that and then you're going to be okay. I don't doubt that in preventing surgical errors, operating on the wrong limb, and that kind of thing, that checklists are very useful. But my real question is to what level? How far should that go?
RW: In computerizing health care, we've seen that alerts designed to cue people to remember that the patient was allergic to medicine, or to do thing x in situation y, are getting ignored because the volume of alerts are such that people feel like they cannot get their work done. Are you familiar with this issue from other lines of work, and what cautions or solutions should we think of around the computerization of patient care?
ET: The false positive problem is one that I hardly have to mention to people interested in patient safety and health care issues, and it's one that also appears in many other safety contexts, for example, the frequency of alarms. One of the issues in fire alarms is that if they go off too often, then it's very hard to get residents of a campus apartment complex to take them seriously. I was in a building like that, and there were so many false alarms that I'm not sure how many people followed what Public Safety tried to get everybody to do, which was to evacuate every time. So an automated system like that does run the same risks, and I don't have a recommendation for dealing with that. But when you look at accounts of many other kinds of accidents, it often turns out that there was a signal; there was a sign warning of something, but people were used to disregarding it. There is another sociological element, and I hope it isn't widespread in medicine but it is in some other areas, that Harvard Business School professor Scott Snook calls "practical drift"—that is that organizations can start to deviate from established procedures and bend them if in their culture they feel this is really necessary to get things done. Snook was himself a victim of a friendly fire episode, and his experience made him really interested in how organizations go wrong when they are supposed to be as accurate and precise as humanly possible, and his theory emerged from his experience. So I think the combination of a high frequency of alarms and pressure for productivity is potentially dangerous.
RW: Let me turn to solutions, because it does strike me that your work is extraordinarily relevant to what we are doing in health care over the past 10 years, as we've thought about safety and quality problems. The epiphany was to approach these issues as system problems rather than manifestations of individual carelessness or sloppiness—most are good people trying hard and the systems have to be improved. As we think about improving and changing systems, are we always going to be empirically measuring these unanticipated consequences and revenge effects after we're done? Or are there ways to prospectively anticipate that something is likely to fall off the back of the truck and mitigate it before you've created the harm?
ET: It's possible to imagine the categories of problems that can arise through new technologies or new regulations. I was reading about the controversy over a robotic surgery system that requires a certain number of hours for proficiency and that can produce significantly better results if the surgeon is really experienced and adept, but also might have a greater potential for adverse outcomes if they're not fully practiced and careful. There's enough evidence from that kind of system that when it is implemented people can focus on, first of all, whom do you practice on, how do you get that experience, and then second, how much continuing education a doctor should have to use it. Many of these things can be foreseen. Some of them involve interaction between the technological system and organizational systems and the organizational ethic. There is a concept called the "high reliability organization" that you might have encountered, and that has as its exemplar the flight deck of an aircraft carrier, which turns out to be a surprisingly manageable environment despite the unbelievable apparent physical risk of it, because people have been trained and drilled so well, and are also able to interrupt regardless of rank. That's something that medicine has learned and could continue to learn from, that any member of the team, even the lowest rank, can interrupt something that the commanding officer has ordered if they see a potentially unsafe situation. The worst aviation disaster in history, at the Tenerife airport in the Canary Islands in 1987, occurred in part because the pilot was such a respected authority figure in European aviation that his subordinates didn't warn him. So there are various bodies of work, both about organizations and about particular technologies, that would let people stretch their imaginations in thinking of the possible risks of innovations, and then they could be alert to watch for them and to take action earlier rather than to wait until a larger number of events have occurred.
RW: For the physicians, nurses, quality managers who do this kind of work, who are in charge of building new systems, do they need additional training to know about these effects? Is this human factors? Is this engineering? Or do we need an extra person sitting at the table who does this for a living to raise these concerns that we might not think of? We may be too much in the middle of the soup.
ET: I'm not sure if adding another category of professional might not have some revenge effect of its own; that's one of the real problems of the field—when you think you're preventing some unintended consequence, you're actually unleashing another one that could be even worse. In the Gulf oil spill cleanup, we were aware of the damage done by some of the chemicals used against the effects of the Exxon Valdez spill. The analysis of possible unintended consequences is really dependent not on a single body of doctrine or a textbook but on experience in many examples of things going wrong in many domains. It's a form of tacit knowledge. It's something that I have to learn for myself reading into the literature of many different fields, but one of the things that I discovered is when you start following this systematically, you start developing intuitions of the kinds of things that can go wrong. To me it's a little disappointing that the advocates of new technologies under discussion aren't more sophisticated in dealing with these possible unintended consequences. I'm not saying that I think that people should just pull back and not do something new and be paralyzed because there might be some harm, but people could use their imagination more in dealing with the world's complexity.
RW: Do you worry about groupthink? As someone sitting around the table hearing the plan, you can imagine that there probably is someone thinking, "But what about this," or "Isn't this bad thing likely to happen," but then feeling like they're going to be the skunk at the party?
ET: That really depends on the leadership of the group. If there is somebody in charge of the group who really wants to push something through, they might pay lip service to possibilities, but in practice they're going to find ways around them. This seems to have been the case, for example, in the federal Minerals Management Service. In studying some of the recent mine accidents, I found there was an institutional pressure there to have the most optimistic assessment of just about everything. I don't think that they necessarily thought that they were really creating some danger. I think that it's possible for people to believe that a lot of requirements are really just paperwork—that it doesn't matter whether the systems are really adequate. The culture created at the top is more important than any number of experts that you have there. I spoke at a conference of professional safety engineers a few years ago, and these were executives who were responsible for the whole programs of companies. Their role though was really quite limited—they were not really able to say, "I don't think we should do this." Or they could say that, but they did not have the total professional autonomy to stop something in the way that the lowest ranking sailor on a flight deck can stop something.
RW: And so was their role to raise flags?
ET: Their role was to raise flags and make recommendations, and they took it seriously. My sense was that, although none of them complained about senior management or suggested to me that they were denied the ability to get things done, everything depended on the attitudes and the values of the people at the top. Everybody else in an organization will tend to follow the lead of the CEO. This is true in government, and it would be true in industry, and I suspect it would also be true in a medical setting. Hospital managers have to be especially aware of the risks of hierarchic organizations. Tokyo Electric Power Co. engineers warned of a tsunami risk several years ago, but TEPCO executives ignored their recommendations. Japan's culture made it harder to discuss the risk. So it might take a certain kind of consistent courage in all parts of organizations to face potential problems rather than to make a series of optimistic assumptions. I think the problems usually come not because people are greedy or selfish or that they don't care, but that their bias and the pressures on them induce them to take an optimistic view of everything.
RW: I think the socio-cultural phenomenon that you've observed in other industries is what we're going through in health care, and we're trying to figure out how to change it. It's a heavy lift.
ET: I can understand that, and I think there's another dimension in health care. One is patient expectations, which can cut both ways. In some cases, the patients themselves might be interested in procedures or medications that might increase the risk for them. On the other side, there is the widely discussed ability of medical professionals, much more than other professionals, to create demand for their services, and those two interact. I'm not saying that that is necessarily a bad thing; sometimes it's a good thing. It can risk life, but it can also help enhance its quality. Either way, though, it sets medicine apart.
Perspective
Edward Tenner is right. Technology does have reverberations, including unintended consequences, or "revenge effects."(1) While such drawbacks are inherent in technology, our poor understanding of technology in health care is a much larger problem. We don't know enough about products or systems that people use to know what can happen. Compared with ignorance, the revenge effects that are inherent in technology are minor.
When we talk about the safety of medical devices, "safe" implies an expectation that a device will keep us free from harm. How safe are medical devices? Eleven years after the Institute of Medicine report To Err is Human (2), there is ample evidence to indicate that issues with device safety remain substantial and widespread. Here are just a few examples.
- Device recalls are the most valid current measure of device failure. I reviewed 1,573 medical device recalls for the U.S. Food and Drug Administration (USFDA) Center for Devices and Radiologic Health (CDRH) that occurred during January 2006–May 2008. Eight hundred ten (51.5%) had human factors (3) at issue and failed in one or more aspects of reliability, efficiency, or safety. For example, software malfunction prevented a defibrillator from delivering shocks when needed. The back of a patient chair on a tomography system bent and broke off, allowing a patient to fall. A ventricular assist device (VAD) permitted implantation of the wrong size nut, causing a poor connection with the inflow cannula that resulted in patient death (Nemeth C, unpublished data).
- Even when the threat from a medical device is known, its solution can still be elusive. In April 2006, members of the surgical team placed an anesthetized patient onto a modular table during preparations for a spinal procedure. While the team adjusted the table, it swung loose and the patient fell to the floor but sustained no injury. The surgical department was aware of the table's flaws, but was willing to trade off the table's safety issues with the unit's features that they felt made it desirable to continue its use. Warranty and USFDA approval concerns precluded the hospital from modifying the equipment. The hospital developed a report of the event for the manufacturer. It also produced a brief improvement plan that included training surgical care team members and hanging a warning sign from the lever on the side of the table's head end control housing. The sign was not used. The table and its inherent safety problems remained in use.(4)
- A recent article on the danger presented by interchangeable intravenous and feeding tubes (5) generated a series of simple, presumptive solutions (6) pointing in directions that could almost be predicted, from clinicians (label the tubes; don't replace trained practitioners with others who are less qualified), to a government agency (we're on it), and a trade organization (have the government mandate bar codes).
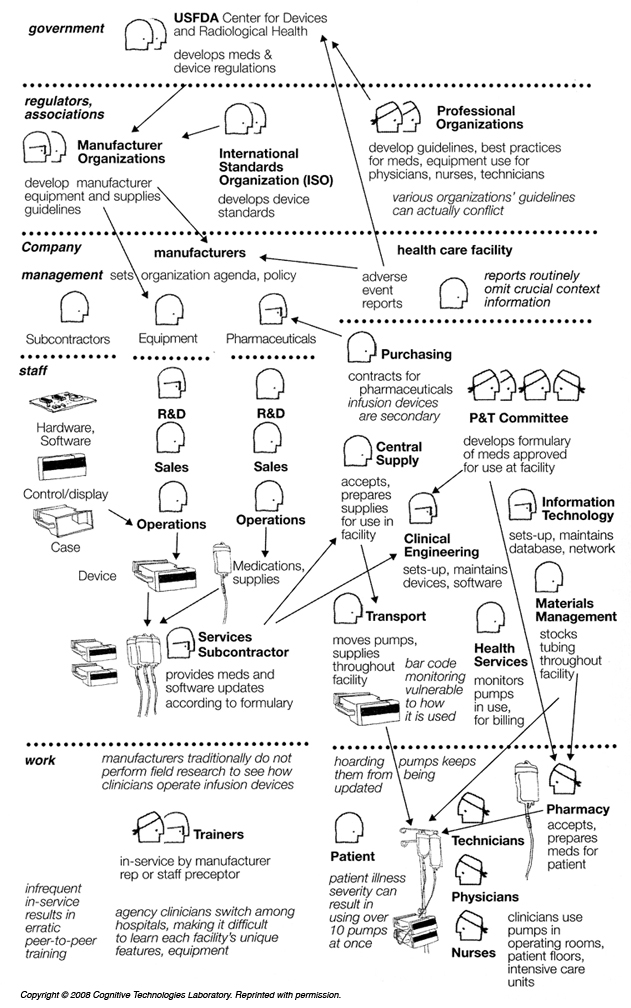
While notions about solutions are simple, the problem and its context are complex. In all of the above examples, the "device" does not stand alone, but is instead part of a larger system that influences its use and effects on patient care and outcomes. The Figure illustrates how an infusion "device," the most widely used information technology (IT) in health care, is actually an interdependent network of relationships. It's a socio-technical system that spans all who develop, supply, and use the result, from the level of the care provider or manufacturer organization, to associations and regulators, to government. This requires a different approach to safety: at the systems, not the device, level.
Complex systems have properties of operation and failure that require study.(7) Health care is a complex sector, with complex phenomena that make it more difficult to generate reliable evidence.(8) Health care continues to resist study for a number of reasons. Departments are separated and teams resist scrutiny. Organizations are pressured to maximize revenue by operating at, or near, saturation. Devices increase in complexity and new versions replace them frequently. Even if we did understand today's version of hardware or software, tomorrow's version will soon come along to replace it. The training that care providers receive about devices is protracted and designed to show what to do when things go right, and omits what to do when they go wrong. Reporting systems abound but lack data collection standards and robust evaluation processes that might make them useful. Too few clinicians question the effect a new technology may have on the patient. Too few manufacturers invest in understanding human performance and how to accommodate operator needs and abilities. Oversight by government agencies is impeded because they are obliged to respect what they are and are not authorized to do, such as oversee devices that are already in the market.
The safety of medical devices relies on well-informed attention and action at all of these levels. Being "well-informed" starts with having good data—a genuine understanding of the real world. As of now, we don't know what can go wrong when devices are in use because there are no data on how the elements in each system interact, and how that affects human performance. A 5-year study of infusion devices showed that junior and experienced clinicians alike routinely got "lost in menuspace" when operating these devices.(9) If the design of a single device such as an infusion pump is a challenge, consider interconnected software including computerized physician order entry (CPOE), electronic medical records (EMR), bar code medication administration (BCMA), and electronic medication administration record (EMAR). These systems are far more complex than a lone pump. They also blur boundaries within and across the organization that were previously clear-cut, and they can hide and propagate far more threats than a single infusion device.
These shortcomings can be avoided with good design, based on good research. Other industries such as aviation do this successfully, but it takes a significant investment to get the benefit. Moving forward starts with systems thinking at all levels: care providers, companies, regulators/associations, and government. That requires an understanding of how complex systems work (7), and how to authentically account for human performance.(10) It also requires what Sterman (11) described as understanding how all models are wrong, a humility about the limitations of our knowledge, and a commitment to the rigorous and disciplined use of scientific inquiry skills.
Without data on human cognitive performance in health care and how technology affects it, we have no information on what the real world of health care is like, and any efforts to improve it are just a collective guess.
Christopher Nemeth, PhD, CHFPPrincipal ScientistGroup Leader, Cognitive Systems EngineeringCognitive Solutions Division of Applied Research Associates, Inc.
Acknowledgement: The author is grateful to Robert Wears, MD; Shawna Perry, MD; Richard Cook, MD; and Jay Crowley for their insightful comments during the development of this essay.
References
1. Tenner E. Why Things Bite Back: Technology and the Revenge of Unintended Consequences. New York: Random House; 1997. ISBN: 9780679747567.
2. Kohn L, Corrigan J, Donaldson M, eds. To Err is Human: Building a Safer Health System. Washington, DC: National Academies Press; 2000. ISBN: 9780309068376.
3. Nemeth C. Human Factors Methods for Design: Making Systems Human-Centered. Boca Raton, FL: CRC Press; 2004. ISBN: 9780415297981. [Available at]
4. Nemeth C, Dierks M, Patterson E, et al. Learning from Investigation. Proceedings of the Human Factors and Ergonomics Society Annual Meeting, San Francisco. October 2006. [Available at]
5. Harris G. U.S. inaction lets look-alike tubes kill patients. New York Times. August 21, 2010:A1.
6. Letters: How to reduce tube mix-ups in hospitals. New York Times. August 25, 2010:A26.
7. Cook RI. How complex systems fail. In Allspaw J, Robbins J, eds. Web Operations: Keeping the Data On Time. Sebastopol, CA: O'Reilly Media; 2010. ISBN: 9781449377441. [Available at]
8. Nunnally M, Nemeth C, Brunetti V, et al. Lost in Menuspace: User Interactions with Complex Medical Devices. In Nemeth C, Cook R, and Woods D, eds. Special Issue on Studies in Healthcare Technical Work. IEEE Transactions on Systems, Man and Cybernetics—Part A. 2004;34:736-742. [Available at]
9. Pew R, Mavor A, eds. Human System Integration in the System Development Process: A New Look. Committee on Human-System Design Support for Changing Technology. Washington, DC: The National Academies Press; 2007. ISBN: 9780309107204. [Available at]
10. Sterman JD. All models are wrong: Reflections on becoming a system scientist. Syst Dynamics Rev. 2002;18:501-531. [Available at]
11. Sterman JD. Learning from evidence in a complex world. Am J Pub Health. 2006;96:505-514. [go to PubMed]
12. Nemeth C, Cook R. The infusion device as a source of resilience. In Nemeth C, Hollnagel E, Dekker F, Dekker S, eds. Resilience Engineering Perspectives, 2. Farnham, UK: Ashgate Publishing; 2009. ISBN: 9780754675204. Preparation and Restoration; vol 2.
Figure
Infusion Device as a Socio-Technical System.(12)
(Go to figure citation in the text)
Click to enlarge.
Copyright © 2008 Cognitive Technologies Laboratory. Reprinted with permission.